Medicare Programs
Behavioral Health
Integration
Behavioral health screening and collaborative care in primary care settings
- PHQ-9 and GAD-7 automated screening
- Collaborative care model with psychiatric consultant
- Integrated in primary care — no separate referral
Overview
What Is Behavioral Health Integration?
BHI supports assessment and management of behavioral health conditions within primary care settings. Using validated screening tools like PHQ-9 and GAD-7, BHI enables primary care providers to deliver depression screening, anxiety management, and substance use disorder monitoring with psychiatric consultation support.
- PHQ-9 and GAD-7 automated screening
- Crisis intervention protocol support
- Medication adherence tracking
- Collaborative care model documentation
PHQ-9
Depression
6.2
↓ avg
GAD-7
Anxiety
5.8
↓ avg
PROMIS-10
Global Health
32.1
↑ avg
Falls Risk
Assessment
Low
→ avg
Eligibility
Qualifying Behavioral Conditions
BHI covers behavioral and mental health conditions managed within primary care. Each condition uses validated screening instruments for evidence-based assessment and progress tracking.
Major Depressive Disorder
F32.xPersistent depressive episodes affecting mood, energy, and daily functioning. Scored via PHQ-9 to track severity and treatment response over time.
Generalized Anxiety Disorder
F41.1Chronic excessive worry and tension affecting concentration and sleep. GAD-7 quantifies severity and guides treatment escalation decisions.
Bipolar Disorder
F31.xAlternating manic and depressive episodes requiring ongoing mood monitoring. PHQ-9 tracks depressive phases; MDQ screens for manic episodes.
PTSD
F43.1xTrauma-related intrusive thoughts, avoidance, and hyperarousal. PCL-5 measures symptom clusters and treatment progress over time.
Substance Use Disorders
F10-F19Alcohol and drug use disorders affecting health and recovery. AUDIT-C screens alcohol use; DAST-10 evaluates drug use severity.
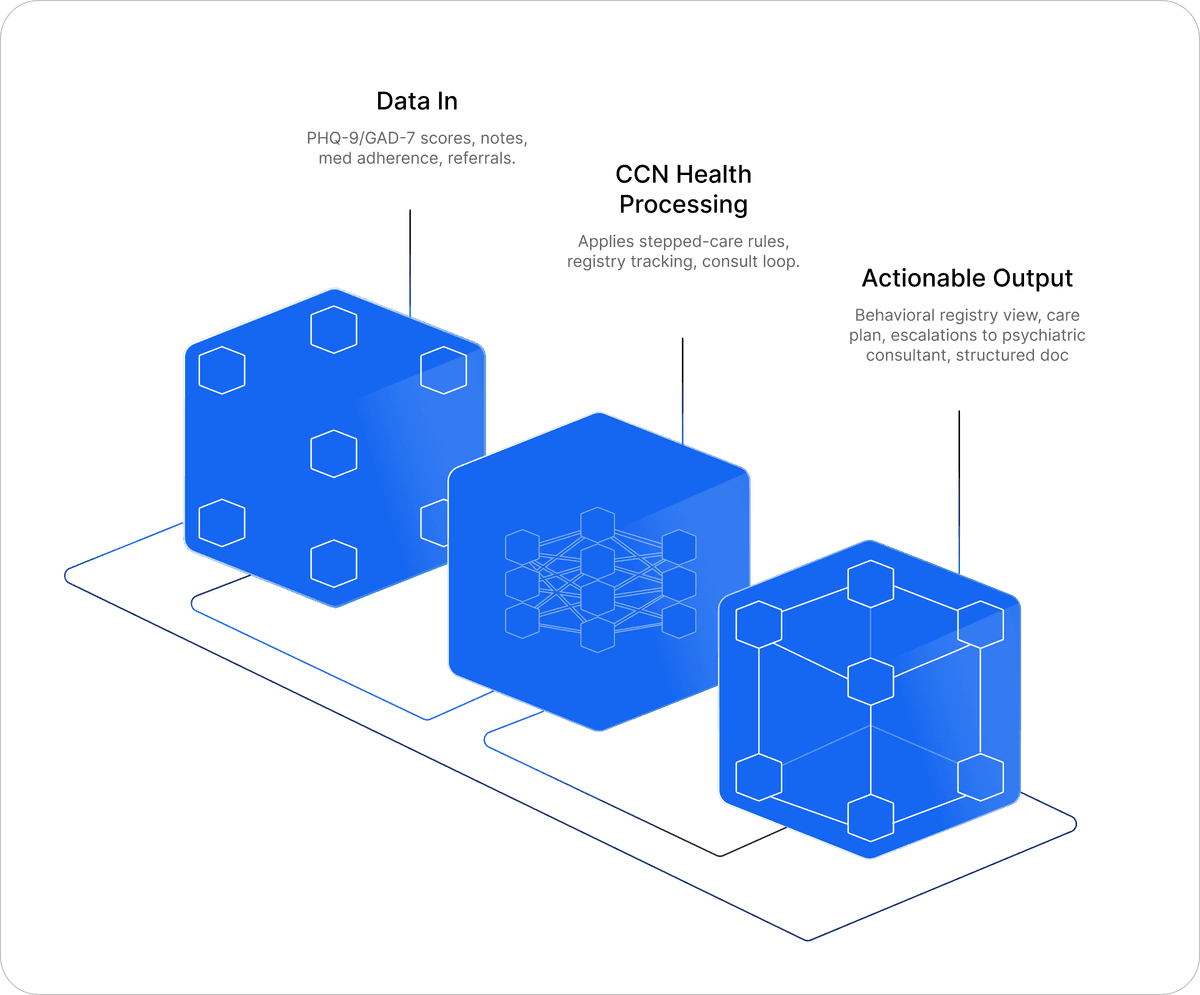
How It Works
BHI Care Delivery Model
A four-step process that integrates behavioral health screening and collaborative care into primary care workflows.
Screen & Identify
Administer validated screening instruments (PHQ-9, GAD-7, AUDIT-C) during primary care visits to identify patients with depression, anxiety, or substance use disorders.
Establish Care Plan
Create a behavioral health care plan with measurable treatment goals, target screening scores, and evidence-based intervention strategies for each identified condition.
Collaborative Care
Care manager coordinates with a consulting psychiatrist for systematic case review. Registry-based tracking ensures treatment adjustments reach patients who are not improving.
Monthly Management
Deliver 20+ minutes per month of behavioral health activities: care coordination, medication adherence tracking, crisis protocol monitoring, and progress documentation.
Platform
Sleep Quality & Behavioral Monitoring
Track sleep patterns — the one physiologic signal relevant to behavioral health. Poor sleep correlates with depression severity, anxiety, and substance use recovery outcomes.
- Sleep quality scoring and trends
- Correlation with screening scores
- Nocturnal pattern analysis
- Behavioral health progress tracking
--
Duration
--
Sleep Score
--
Resting HR
--
Resp Rate
5
Behavioral Conditions
20
Minutes Monthly Minimum
3
Billable CPT Codes
$48
Base Monthly Revenue
Revenue
CPT Codes & Billing
BHI offers two billing tracks: general care management (99484) and the higher-revenue Collaborative Care Model (CoCM) with psychiatric consultation.
BHI Care Management
General BHIGeneral behavioral health care management. No formal CoCM required. Covers assessment, care planning, and ongoing management of behavioral health conditions.
~$49
Monthly
20+ min clinical staff time
Initial Psychiatric Collaborative Care
CoCM (Higher Revenue)Initial month of the Collaborative Care Model (CoCM). Requires behavioral health care manager + consulting psychiatrist. Highest single-month BHI reimbursement.
~$163
First month
70+ min first month
Subsequent Collaborative Care
CoCM (Higher Revenue)Ongoing monthly CoCM management after the initial month. Includes systematic case review, treatment adjustment, and psychiatric consultation.
~$130
Monthly (subsequent)
60+ min subsequent months
CoCM = Higher Revenue Track
Practices with a consulting psychiatrist and dedicated behavioral health care manager can bill 99492/99493 instead of 99484, increasing monthly per-patient revenue from $48 to $130–163. The CoCM model is the recommended path for maximizing BHI program value.
Why CCN Health
Purpose-Built for Behavioral Health
BHI is the most clinically different Medicare program. Our platform is designed specifically for behavioral health workflows, not retrofitted from vital-sign monitoring.
Validated Screening
PHQ-9, GAD-7, AUDIT-C, and DAST-10 screening instruments are built directly into the platform. Automated scoring eliminates manual calculation errors and ensures consistent, evidence-based assessments across your entire patient panel.
Collaborative Care Model
Structured CoCM workflows connect your care manager with a consulting psychiatrist for systematic case review. Registry-based tracking ensures no patient falls through the cracks, and the higher-revenue 99492/99493 codes become accessible.
Progress Tracking
Standardized outcome measurement over time with trend visualization. Track PHQ-9 and GAD-7 score trajectories to demonstrate treatment response, identify patients who need escalation, and document measurable improvement for payers.
Primary Care Integration
Behavioral health screening embeds directly within existing primary care workflows. No separate behavioral health referral required. Patients receive mental health support in the same setting where they already receive medical care.
Crisis Protocols
Automated escalation pathways for acute risk detection. When screening scores indicate suicidal ideation or severe symptoms, the platform triggers crisis intervention protocols and alerts the supervising clinician immediately.
Compliance Documentation
Every screening administration, score calculation, and care coordination activity is automatically documented with timestamps. Assessment-backed records support every BHI claim and provide audit-ready documentation for Medicare compliance.
Compliance
Common Pitfalls & Compliance Notes
Avoid costly billing mistakes and stay audit-ready with these BHI compliance guidelines.
Common Mistakes
- 01Billing 99484 without adequate documentation of a psychiatric collaborative care model or behavioral health management framework
- 02Not meeting the 20-minute minimum clinical staff time requirement for the calendar month
- 03Insufficient behavioral health documentation — generic care coordination notes do not satisfy BHI requirements
- 04Failing to use validated screening tools (PHQ-9, GAD-7) for initial assessment and progress monitoring
- 05Not clearly identifying the behavioral health condition being managed in the care plan
- 06Confusing BHI (99484) with Psychiatric Collaborative Care Model codes (99492-99494), which have different requirements
Compliance Notes
- BHI (99484) is a general behavioral health care management code — it does not require a formal Psychiatric Collaborative Care Model (CoCM), though it can complement one
- For practices with a structured CoCM program (consulting psychiatrist + behavioral health care manager), consider codes 99492-99494 instead, which reimburse at higher rates
- BHI can be billed concurrently with RPM if the patient has both behavioral health and physiologic monitoring needs
- BHI should not be billed in the same month as CoCM codes (99492-99494) for the same patient
- Clinical staff providing BHI services must have appropriate behavioral health training and credentials
- Progress must be documented using standardized tools — clinical judgment alone is insufficient for compliance
FAQs
Frequently Asked Questions
Common questions about BHI eligibility, billing, and program implementation.
BHI (99484) is a general behavioral health care management code that can be billed by any practice providing structured behavioral health services. Psychiatric Collaborative Care codes (99492-99494) require a formal collaborative care model with a designated behavioral health care manager and a consulting psychiatrist. CoCM codes reimburse at higher rates but require more infrastructure. Practices without a consulting psychiatrist typically use 99484.
Yes, BHI can be billed concurrently with CCM and/or RPM for the same patient, provided that the time and services are distinct and not double-counted. For example, a patient with diabetes (CCM) and depression (BHI) could receive both services in the same month. The BHI time must be specifically focused on behavioral health management, while CCM time covers the chronic medical conditions.
While CMS does not mandate specific tools, industry standards include: PHQ-9 (Patient Health Questionnaire) for depression, GAD-7 (Generalized Anxiety Disorder scale) for anxiety, AUDIT-C for alcohol use, and the DAST-10 for drug use. Using validated tools demonstrates evidence-based care and supports medical necessity. Assessments should be administered at baseline and at regular intervals to track treatment response.
BHI services (99484) can be provided by clinical staff — including licensed clinical social workers, psychologists, registered nurses, and other qualified behavioral health professionals — under the direction of the billing physician or qualified healthcare professional. The billing practitioner must establish the behavioral health care plan and oversee the clinical staff providing the services.
Yes, substance use disorders (SUDs) are qualifying behavioral health conditions for BHI. Services can include screening with validated tools (AUDIT-C, DAST-10), care plan development for recovery support, medication-assisted treatment coordination, and ongoing monitoring. BHI provides a reimbursement pathway for primary care practices managing patients with SUDs who may not have access to specialized addiction medicine providers.